
Physicians who perform skin rejuvenation are constantly inundated with information about new devices that offer photodamage reduction and elasticity restoration—but without the recovery or risks inherent with ablative lasers or aggressive chemical peels.
Many of these devices are truly novel, whereas others are simpler, older technologies that have been applied in new ways.
The claims made by device manufacturers, some practitioners, and the media have made it extremely difficult for the clinician to adequately judge efficacy and to discern purported differences among devices.
Moreover, obtained clinical results, although often leading to patient satisfaction, are often not clinically significant in the mind of the treating physician.
With age, there is a loss of a person’s normal elastic fibers and function, as well as changes in collagen and collagenase activity. However, solar exposure and resultant photodamage appear to be more significant than chronological aging in producing the typical changes associated with “aged” skin.
 |
 |
| Microdermabrasion has long been the gold standard among approaches used for mechanical exfoliation of the stratum corneum. | |
Chronic ultraviolet exposure produces histologic evidence of solar elastosis, an accumulation of abnormally oriented elastic material in the superficial to mid dermis. This replaces the normally arranged collagen and elastic fibers.
In addition, chronic sun exposure causes both a decrease in collagen and a disruption of normal morphology and fiber organization. The resultant clinical effects of altered collagen and elastic fibers are sagging, wrinkling, furrows, and pigmentary and texture changes.
Where We Are Now
Currently, you can use myriad methods to treat photodamaged skin. These include topical agents such as retinoic acid, various peels, dermabrasion, and laser resurfacing.
These treatments correct chronic photodamage through somewhat similar—albeit different—mechanisms, which all lead to some form of trauma to the dermis. The biological response to this trauma leads to deposition of a new extracellular matrix.
In addition, the healing process leads to more normally oriented collagen and elastic fibers, and a thickened grenz zone separating the dermis and epidermis.
Topical agents, such as retinoic acid, are somewhat effective but are not able to elicit enough of a response to correct deep furrows and wrinkles.
Microdermabrasion has long been the gold standard among approaches used for mechanical exfoliation of the stratum corneum.
Since its introduction in the United States in the mid 1990s, microdermabrasion has played an integral role in the creation of today’s aesthetics industry. Holding its popularity among the top five nonsurgical, cosmetic procedures, more than 850,000 patient treatments were done in 2007.
Stand-alone microdermabrasion has proved to be extremely effective in treating a variety of conditions, including acne, superficial epidermal pigmentary changes, and photoaged skin.
The technique is an integral part of an overall healthy skin care regimen for sun-damaged skin, fine lines, wrinkles, solar lentigines, enlarged or oily pores, comedonal acne, mild acne scars, and melasma.
Microdermabrasion is also indicated as a pretreatment for many light- and laser-based treatments. In fact, pretreatment with microdermabrasion used as an adjunct to photodynamic therapy has shown to increase permeation of 5-aminolevulinic acid up to 15 times.
The continued popularity of the microdermabrasion procedure has led investigators to look for ways to enhance treatments.
With the idea that the microdermabrasion-treated stratum corneum can be altered to reduce its ability to perform as a barrier, physicians grew interested in the ability to propel topical products into the skin during or following a microdermabrasion treatment.
 |
 |
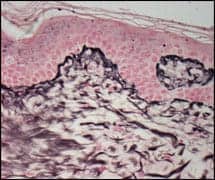
| Figures 1 and 2. Treatment was tolerated well by all patients, with only mild erythema observed in the immediate postprocedure period. | |
New Suffusion Research
One of my research programs recently completed a study using ultrasound phonophoresis to infuse a topical solution immediately following a microdermabrasion treatment.
The objective was to bring about microdermabrasion-induced changes in the skin by creating cytokine pathways through which cosmeceutical ingredients can pass, allowing them to bring about change in the subepidermal layers.
With that in mind, the following protocol was undertaken: Seven patients underwent eight weekly treatments of microdermabrasion, with each treatment followed by ultrasound phonophoresis administration of a hyaluronic acid, retinol, and peptide-containing complex.
Hyaluronic acid is a humectant. For years, humectants have been used in cosmetic products. Humectants pull water from the deeper epidermal and dermal tissues to rehydrate the stratum corneum.
Humectants may allow the skin to feel smoother by filling holes in the stratum corneum via hydration. This hydration may allow other associated cosmeceutical agents to better penetrate the skin.
Retinol is the naturally occurring vitamin A form found in red, yellow, and orange fruits and vegetables. It can be oxidized to retinaldehyde and then oxidized to retinoic acid, also known as prescription tretinoin.
This cutaneous conversion of retinol to retinoic acid is responsible for the biologic activity of some of the new, stabilized over-the-counter vitamin A preparations designed to improve the appearance of benign photodamaged skin. Unfortunately, only small amounts of retinyl palmitate and retinol can be converted by standard topically applied retinol.
Cell-permeable synthetic peptide-containing complexes have been shown to control subcellular traffic of transcription factors that can mediate cellular responses to different agonists.
Any method that helps to propel retinol and peptide-containing complexes into the skin, in theory, may lead to increased dermal collagen production.
In the research program, all subjects were assessed at baseline and at 3 months following the last treatment. Clinical evaluation included pretreatment and post-treatment high-quality digital photography, as well as subject and investigator assessment of changes in skin dryness, texture, hue/brightness, tone, and rhytids.
Improvement was graded on a zero- to nine-point scale, using the following criteria:
- Dryness (zero was very dry; nine was very moist);
- Texture (zero was very rough; nine was very smooth);
- Hue/brightness (zero was a dull, matte finish; nine was a bright, radiant finish);
- Tone (zero was a very blotchy, uneven finish; nine equaled no blotchiness, and an even color); and
- Rhytids (zero equaled none; nine was numerous).
Three months following the last treatment, the subjects were asked to rate their improvement in the same categories using the same scale.
Data was analyzed and assessed as the percentage of patients with a certain point improvement. Histologic evaluation consisted of pretreatment and post-treatment 3-mm punch biopsies of preauricular skin evaluated for microscopic and ultrastructural changes.
Treatment was tolerated well by all patients, with only mild erythema observed in the immediate postprocedure period. No edema or purpura was observed.
Throughout the follow-up period, no persistent erythema, edema, postinflammatory pigment alteration, purpura, or scarring was noted in any of the treated individuals.
Clinical improvement was seen in the various signs of photodamage, assessed as a percentage of patients showing a particular point improvement in the various signs of photodamage, evaluated by either the subjects themselves or by investigators.
Light microscopic findings demonstrated by methylene blue stain showed increased vascularity within the papillary dermis in the post-treatment biopsies compared with pretreatment specimens, indicating zones of injury and repair.
Increased reticulin staining of Type-III collagen within the papillary dermis provided further evidence of injury and subsequent new collagen deposition (Figures 1 and 2).
Ultrastructural evidence of dermal remodeling was provided by electron microscopic findings of increased collagen fiber diameter, indicating mature Type-I collagen deposition.
|
See also “What’s the Skinny on Plasma Resurfacing?” by Dan Yamini, MD, FACS, in the December 2007 issue of PSP. |
The combined microdermabrasion- and ultrasound-propelled product approach (which is termed suffusion) was painless and can be used for all skin types.
Transdermal Delivery
The idea of transdermal delivery of cosmeceuticals is not new.
Countless recent cosmeceutical products contain new and promising active ingredients.
The challenge to physicians is how best to deliver these products below the epidermal barrier, where they will be most effective.
David J. Goldberg, MD, JD, is a board-certified dermatologist and director of Skin Laser & Surgery Specialists of New York & New Jersey, headquartered in New York City. He also is a clinical professor of dermatology and director of laser research at Mount Sinai School of Medicine and an adjunct professor of law at Fordham Law School, both in New York City. He can be reached at .


