-By Alexander P. Moya, MD
Alexander P. Moya, MD, reflects on the evolution of the corset trunkplasty
More than one-third of US adults are obese, according to the Centers for Disease Control and Prevention. As the obesity epidemic continues, bariatric surgery is becoming an option for more and more people. According to the American Society for Metabolic and Bariatric Surgery, approximately 200,000 bariatric surgeries are performed each year.
Weight-loss surgery is often not the last procedure that such patients will require. Body contouring following bariatric surgery and massive weight loss from other means is an ever-evolving field.
Many of the more popular body-contouring procedures fail to consider the entire abdominal region where hanging fat and flab can cause skin intertrigo and odor, and obscure the waistline.
I began treating these patients with either a wedge abdominal panniculectomy or extended abdominoplasty since many were not interested in undergoing a circumferential belt lipectomy due to the overall cost. I also found myself hesitant to aggressively elevate an abdominal flap in patients who had undergone a previous upper midline incision from an open gastric bypass or other bariatric procedure due to the possibility of a major wound complication.
Unfortunately, this conservative approach left many of these patients with a less-than-desirable body shape.
The Corset Trunkplasty Begins to Take Shape
To better meet their needs and improve satisfaction, I began utilizing a fleur-de-lis technique to address both the horizontal and vertical skin redundancies. With this approach, I would easily be able to incorporate a wedge panniculectomy (covered by insurance), utilize a previous upper midline incision, and limit overall complications by eliminating undermining of tissues for closure.
I realized that the greatest change in waistline shape was afforded by reducing the horizontal skin redundancy with the vertical resection, and thus this became the first and most important step of the modified procedure. This led to completing all of my preoperative markings in the supine position after prepping and draping. I also started utilizing a tailor-tacking method for marking the skin to be resected, a technique which is completed in a sequential fashion throughout the procedure for maximal contouring. By directly excising redundant tissue where it lay and simply closing the defect by pulling the lateral skin edges together, wound complications were minimized.
I was able to obtain impressive lower waistline shape with the use of a vertical approach, but I felt that the upper waistline was still not being adequately addressed. The residual redundancy along the upper abdomen was being accentuated by the “dog ear” created by the midline closure. As a result, I decided to incorporate a third incision along the lower chest (inframammary folds in women) to address the mid-trunk region (upper abdomen and lower chest). The addition of this reverse abdominoplasty-type of resection resulted in a final on-table “corset-appearing” waistline and gave rise to what I eventually called the “corset trunkplasty.”
 |
 |
The Corset Body Lift is Born
The corset trunkplasty (also now known as The Corset Body Lift) comprehensively addresses the abdominal and waistline regions in a single stage, with particular attention to creating an hourglass figure in women. It has become the cornerstone massive-weight-loss body-contouring procedure in my practice. It not only directly resects redundant skin along the anterolateral trunk, but its primary closures also indirectly affect the posterior waistline, thereby resulting in a 360o improvement.
This procedure has successfully reshaped 140 patients (133 women) over a wide BMI range (19½ to 50½) in the last 6 years, many of whom had experienced massive weight loss (157 pounds, on average) due to gastric bypass. (Of note, more than half of these patients had undergone a laparoscopic approach and thus did not have a previous midline incision.)
My current approach to the corset trunkplasty does not require the use of a postoperative drain. I attribute these both to the lack of undermining as well as improvements in my overall technique. I exclusively utilize ultrasonic (Harmonic™) technology for all resections, which helps to minimize surrounding tissue damage and seal lymphatic channels. In addition, bidirectional barbed sutures allow for tighter and motion-free closures. This drain-free technique has been utilized in approximately 60 cases, all without development of a single seroma.
The procedure takes 3½ to 6 hours to complete depending on the degree of skin redundancy, overall body size, and contouring objective. It is routinely performed on an outpatient basis, usually requiring only one overnight hospital stay. Postoperative compression is encouraged, and strenuous activities are restricted for 6 weeks.
Reflections on a Decade’s Worth of Procedures
In my experience with the corset trunkplasty, I have seen an overall complication rate of approximately 30%. The majority of these complications are minor, and include superficial wound dehiscence and small areas of skin necrosis, both requiring only local wound care. Since the surgical technique usually averages 4 to 5 feet of incisions and 10 pounds of skin removal, I believe that these minor complications are very acceptable and do not affect the extremely positive outcomes.
The corset trunkplasty provides great versatility in treating a large range of weight-loss patients from the ideal to the more complex with multiple skin rolls. It has allowed me to address specific areas of skin redundancy (such as the abdomen only, or to include the upper and/or lower back). I can also help those patients who are financially restricted since I can limit the length and/or adjust the position of one or both transverse incisions. This overall flexibility of the corset trunkplasty has allowed me to treat a far greater number of patients.
It has been a decade since my initial frustration as a new attending trying to manage the contouring difficulties of the growing number of massive-weight-loss patients presenting to my office. With the corset trunkplasty, I now have the technique necessary to successfully treat complex body deformities due to multidimensional skin redundancy, both safely and reliably. This subset of patients now makes up 50% of my practice, and has become very satisfying and rewarding. Over the years, these patients have taught me that they are ultimately interested in a procedure that can provide the most significant improvement in body shape (with emphasis on the abdomen and waistline), and as a result, can easily look beyond complex and lengthy scars.
I continue, however, to face the challenge of convincing my colleagues that the perception of optimal aesthetics in this group of patients can be obtained with this aggressive technique, and I look forward to doing so, even if it means one surgeon at a time.
Step-by-Step Guide to the Corset Trunkplasty
1) In the supine position, skin is prepped from the sternal notch down to the upper thighs and from side-to-side, which includes part of the back.
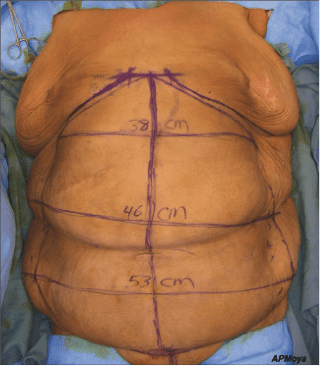
2) All preoperative markings are then completed, which consists of the vertical midline, lower chest, and pubic reference lines.
3) The horizontal skin redundancy extending from the costal margins to hips is pulled toward the midline, inverted and temporarily stapled; the stapled skin is then marked and released.
4) The marked areas are then connected to one another on each side and to the top and bottom of the preoperative midline reference line, forming a large vertical ellipse. This tailor-tacking step is performed as aggressively as possible to maximize skin removal, while at the same time the rolled-up tissue to be excised provides a built-in margin of safety for closure without undermining.
5) Several transverse “hash lines” are then drawn across the vertical ellipse to aid in closure, and the preoperative lower chest and pubic reference lines are partially incised and restapled in order to maintain their positions for future identification.
6) The ellipse is then resected off the abdominal wall and the large defect closed by pulling the lateral skin edges together.
7) The second resection is performed over the lower chest (again utilizing a tailor-tacking marking technique) and, depending on the desired outcome, may be extended onto the upper back. If the procedure is designed to maximize abdominal contouring only, the incision is limited to the anterior chest (limited to removal of the upper midline “dog ear”). Extending the incision to include resection of redundant lateral chest skin will also enhance the upper
waistline contour.
8) The lower chest defect is then closed without undermining by pulling the lateral skin edges together.
9) This is followed by the last resection, which involves the lower abdomen and anterior hips (limited to removal of the lower midline “dog ear”), but can also be extended onto the lower back to enhance the lower waistline contour. The lower trunk resection technique is essentially a mirror image of the resection along the lower chest. While closure of the abdomen requires no undermining, moderate undermining may be safely performed along the hips (inferiorly based
dissection) as needed.
Alexander P. Moya, MD, is the director of the Center for Aesthetics & Cosmetic Surgery and Weight Loss Body Contouring Program for Geisinger Health System in Danville, Pa. He regularly teaches instructional courses on the corset trunkplasty at the annual meetings of the American Society for Aesthetic Plastic Surgery and American Society of Plastic Surgeons, as well as the Geisinger Medical Center. He can be reached at [email protected].
