Monitoring transepidermal water loss and hydration identified high-risk skin flaps within the first three postoperative days, potentially enabling earlier intervention.
Random-pattern skin flaps are frequently used in reconstructive surgery to repair tissue defects, but surgeons still face a difficult question after reconstruction: Which flaps will survive and which will fail? A new study published in Burns & Trauma suggests that the answer may appear in the skin barrier before tissue damage becomes visible.
By tracking changes in water loss and skin hydration, researchers identified early warning signals of flap necrosis and linked them to ferroptosis, macrophage inflammation, and regulatory T cell (Treg) responses. The findings point to a non-invasive monitoring strategy that could help clinicians recognize high-risk flaps earlier and intervene before irreversible tissue loss develops.
Because random-pattern skin flaps receive blood from small subcutaneous vessels rather than a defined main vessel, they are vulnerable to oxygen deprivation and restricted blood flow. Traditional clinical assessments, such as monitoring flap color, swelling, and texture, can be subjective and often fail to detect issues until tissue damage is irreversible.
Researchers from Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, and several other institutions found that transepidermal water loss and stratum corneum hydration reflect the integrity of the skin barrier. By monitoring these levels, clinicians may identify early signals of necrosis, or tissue death, before it is visible.
Rather than waiting for color changes, swelling, or clear necrosis, clinicians may be able to read the skin barrier as an earlier biological warning, according to the study’s authors.
Barrier Failure Precedes Tissue Death
The study used mouse models and clinical samples to demonstrate that barrier failure precedes overt tissue death. In the clinical analysis, a relative transepidermal water loss greater than 3.5 and relative stratum corneum hydration lower than -2.5 were strong predictors of future necrosis. These changes were most significant within the first three days following surgery, providing a critical window for medical intervention.
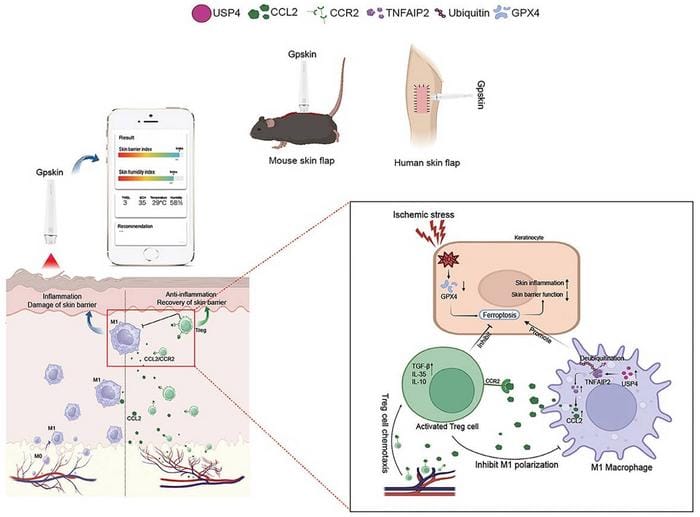
The research also identified the underlying biological mechanisms of this deterioration. Ischemic stress triggers ferroptosis, an iron-dependent form of cell death that damages skin cells and intensifies inflammation. The team discovered that a specific pathway involving ubiquitin-specific protease 4 and tumor necrosis factor alpha-induced protein 2 helps recruit regulatory T cells, which act as a protective counterweight to limit inflammation and tissue damage.
The researchers say the work also explains why that warning appears: Ischemic stress activates ferroptosis and inflammatory macrophages, while the USP4–TNFAIP2 pathway helps recruit Tregs to limit damage.
The authors suggest that a portable skin barrier monitoring approach could guide timely treatment and reduce the need for invasive biopsies or subjective observations. While the results are promising, the researchers note that larger multicenter studies involving different flap types and patients with other health conditions are necessary before the method is widely adopted in clinical practice.
Photo caption: Skin barrier monitoring reveals early signals of flap necrosis.
Photo credit: EurekAlert/Burns & Trauma
