
the face
Sweet Cheeks
The midface rejuvenation revolution
There are few physical attributes that convey youth as much as firm, rounded cheeks. Even minor ptosis or volume loss can produce a drawn and tired-looking appearance, yet midface treatment is too often glossed over during comprehensive diagnosis and treatment of the aging face. Times are changing thanks to the advent of customized implants; better use of existing soft-tissue fillers; and the approval of the first-ever anatomically specific, designer filler: Allergan’s Juvéderm Voluma. 
THE LOWDOWN ON CHEEKS
THAT POP
Many treatment options are available today to add volume to the midface. They all have fans and detractors, and pluses and minuses.
One of the most basic treatments to enhance the midface is silicone cheek implants. The power of this treatment is that it is permanent, yet reversible. With screw fixation to the facial skeleton, these implants will remain in place indefinitely. However, if the patient wants them changed or reversed, the explantation procedure is simple. Facial implants come in a variety of sizes and anatomic shapes, and over the years they have proven to be safe, natural, and effective. They remain a cornerstone of my practice (Figure 1).
Most of us with grey hair (or no hair) have witnessed numerous paradigm shifts in cosmetic surgery. In my career, I have witnessed the advent of liposuction, laser technology, endoscopic surgery, neurotoxins, and, of course, facial fillers. For those surgeons who remember the Zyplast/Zyderm days of bovine collagen, filler treatment was pretty limited back then. No one came into my office in 1995 requesting filler augmentation of the tear trough, cheek, or temple regions. When the federal Food and Drug Administration (FDA) began to approve a steady stream of Hyaluronic acid fillers, which were safe and reversible, surgeons set out to conquer the face. All of a sudden, we were treating—yes—cheeks, chins, jowls, temples, brows, and more instead of just lips and folds.
Today’s contemporary FDA-approved injectable options include Hyaluronic acid fillers, Poly l-lactic acid, calcium hydroxyapatite, methyl methacrylate, silicone oil, and autologous fat, as well as the newly approved Juvéderm Voluma.
CONFESSIONS OF A “FILLER BARTENDER”
I feel that every patient from the late third decade on is a candidate for midface augmentation. My personal approach to filling the midface with some of the older dermal fillers is basically guided by the age of the patient. For patients in their late 30s and early 40s, a single syringe split between both cheeks and superficially injected may be adequate to produce a rounded “cheek apple.” On the other hand, older patients may require multiplanar injection of the cheek with simultaneous injection into the tear trough region and require three to four syringes.
Although I am a “filler bartender,” 99% of my midface filler consists of Hyaluronic acid products. I prefer the larger-particle or more robust formulations such as Perlane and Juvéderm Ultra Plus, but I have successfully used Belotero, Restylane, and Juvéderm Ultra as well. The higher
G prime of these injectables provides more “lift and heft” to support the heavier cheek complex. Radiesse is also a good choice for this region, and Sculptra is popular with numerous colleagues.
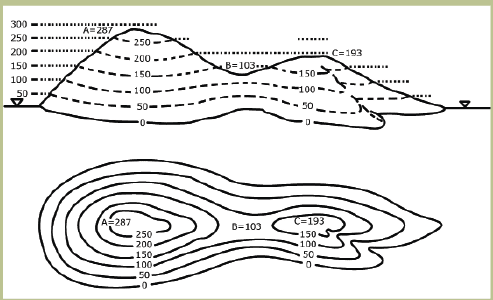
The ability to diagnose and treat the cheeks in three dimensions is mandatory. Consider the topographic map. A topographic map is used to convey a third dimension on a two-dimensional flat map. Contour lines placed on the map represent lines of equal elevation above (or below) a reference datum (baseline). The concentric circles are superimposed so that the larger circles represent lower elevations, and the smallest circles indicate the highest elevations (Figure 2). 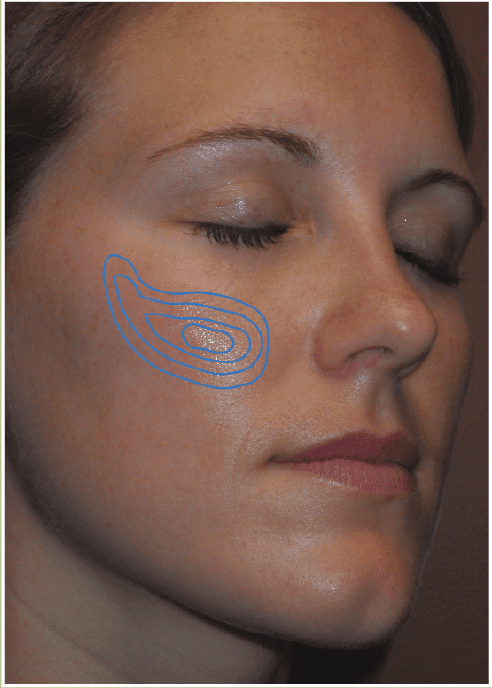
A youthful cheek has this 3D contour with the greatest projection producing the light reflex at the apex of the cheek. This point is sometimes described with measurements (medial to a line from the lateral canthus to the lateral lip commissure), but I think the artistic part of cheek filling is to determine where this point looks best on each patient.
For younger patients, I inject the “upper circles” of the topographic map. Since their volume loss is small, a layer of intradermal injection and dermal injection will produce adequate fill and projection. This can be accomplished by 0.5 mL of Hyaluronic acid filler per side. For patients with moderate volume loss, I include more “topography” and inject more tissue planes. This would include subcutaneous, intradermal, and dermal treatment producing smaller circles toward the apex. This treatment may require 1.5 to 2 mL of filler.
For significant volume loss, I add more “circles”—thus, the maximum multiplanar treatment. This includes periosteal injection, subcutaneous injection, subdermal, and dermal injection to provide a supported foundation with filler in the entire cheek complex. These patients may also require simultaneous tear trough filling to perfect the result. In reality, even moderate midface volume loss can involve tear-trough filling. I refer to the complex as the “cheektrough,” as the cheek blends into the tear trough.
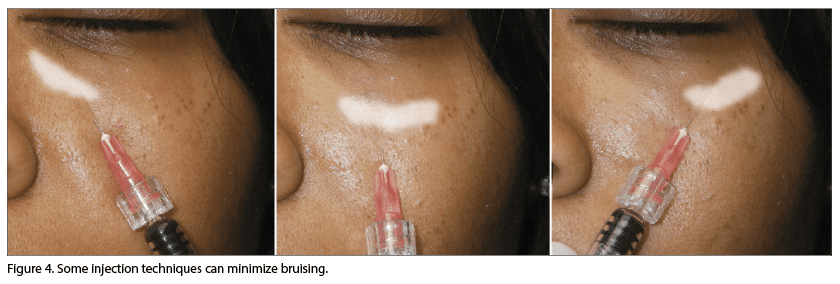
As for treating the tear trough region (nasojugal groove), I originally injected in the depth of the trough to the level of the periosteum. This approach was less predictable in my hands and often led to significant bruising. I began approaching the tear trough from ½ inch inferior to the center of the trough. Using a ½-inch needle, this approach is through the thick cheek skin instead of the thin and fragile lower lid skin. This approach puts the bevel of the needle directly into the tear trough.
I no longer inject on the periosteum, but rather in a plane below the orbicularis oculi muscle. This more superficial deposition of filler improved my results dramatically, and the lower entry has greatly reduced bruising. In addition, I can fill the entire tough from a single puncture in the upper cheek. The needle tip can be directed through the single needle stick to reach the central, lateral, and medial tear trough without withdrawing all the way (Figure 4). The filler can also be “walked” medially by finger pressure. The gel filler in this fine tissue is very easy to move through the tissue, and this can push filler in the medial trough while keeping the needle away from ominous vessels. Less is more when filling tear troughs. 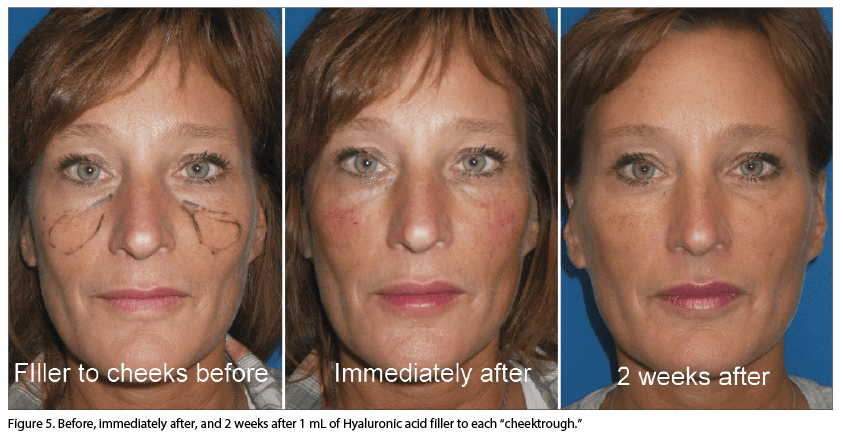
GAME CHANGE: FIRST DESIGNER FILLER ENTERS US MARKET
September 2013 brought about the first FDA filler approved specifically for cheek augmentation. Juvéderm Voluma by Allergan is the first “designer” filler to hit the market, and it will surely be followed by other “anatomic specific” fillers. Use of Voluma requires a different approach and technique than some of its predecessors.
Voluma’s properties are based around Allergan’s Viacross cross-linking technology. This cross-linking produces a filler with a high G prime for viscosity and support, but it also produces a less hydrophylic material. This means that less fluid is pulled into the tissues, which produces a “what you see is what you get” result with less postinjection edema.
Voluma is a moldable filler, and it is best injected deep into the tissues with the ½-inch, 27-gauge needle perpendicular to the skin surface. Due to the properties of this filler, a little bit goes a long way. Generally, one to two syringes will treat most patients. For significant volume loss, I begin just above the periosteum and end just below the dermis.
Voluma is not a dermal filler, and it is not indicated for wrinkles, folds, and tear trough injection. Our Canadian colleagues who have been using Voluma for years say that “topping off” the treatment at about 8 to 9 months can maintain a result for up to 18 months. Other advice from experienced users is that Voluma is more resistant to hyaluronidase when compared to other Hyaluronic acid-based fillers and may take more enzyme to dissolve.
Newer options as well as better understanding of how to use some of the existing treatments will increase the popularity of midface rejuvenation procedures. I predict that minimally invasive filling of cheeks and tear troughs will rise as one of the most requested rejuvenation procedures in the hands of all specialists who provide cosmetic facial treatments.
Joseph Niamtu III, DMD, is an oral and maxillofacial surgeon with a practice limited to cosmetic facial surgery in Richmond, Va. He also serves as a member of the Plastic Surgery Practice editorial advisory board. He can be reached at [email protected].
Original citation for this article: Niamtu, J.. Sweet cheeks, Plastic Surgery Practice. 2014; January: 20-23
