
 |
| Figure 1. Volumetric stacking of soft tissue. (Click for larger image) |
Understanding facial aging, for the aesthetic surgeon, has evolved into a comprehensive analysis and surgical plan that includes both vector and volume correction.
The central oval of the face was largely unaffected by peripheral approaches to this key area. Central to facial aging in the middle third is the descent of the malar fat pad.
This subcutaneous structure becomes ptotic with age, gravity, etc.
There have been multiple approaches in an attempt to reliably elevate this structure with concomitant shortening of the lid/cheek junction and improvement of the nasolabial fold.
Certainly, the midface—from the lower eyelid to the oral commissure—can be approached peripherally. Whether or not the dissection is subcutaneous or subfascial (subSMAS), the appropriate vector must be applied to elevate the midface.
A pure subcutaneous approach, without either performing a subSMAS dissection or a SMASectomy, is unlikely to improve the midface unless the dissection is taken quite anteriorly, so that the malar fat pad may be directly elevated and sutured superiorly and laterally.
A high SMASectomy or SMAS dissection can provide vector-based correction of midface ptosis and may restore volume to the deflated midface.
 |
 |
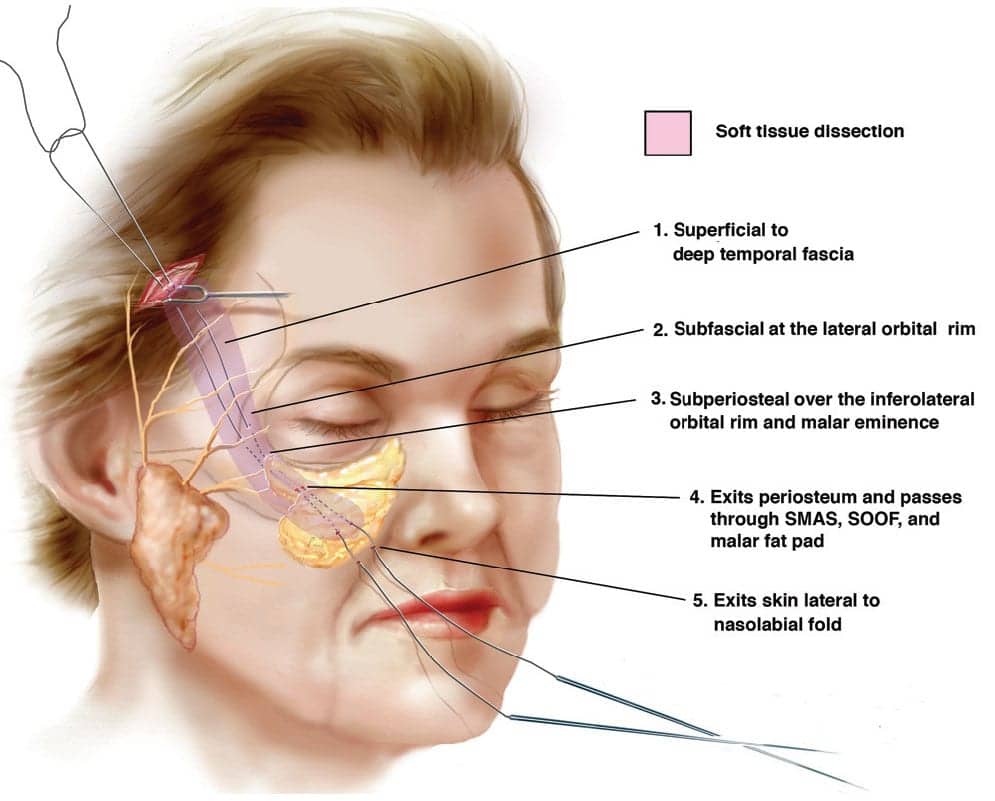
| Figure 2. Soft tissue dissection. (Click for larger image) | Figure 3. Deployment of threads. |
A DIRECT APPROACH
A transpalpebral approach, traversing the midlamella of the lower eyelid, is a direct approach to the midface, but it may be associated with significant morbidity if the lower eyelid is inadequately supported to the lateral orbital rim.
I have moved from the transpalpebral approach to the combined transtemporal/transbuccal approach in order to avoid issues related to the lower eyelid.
 |
| Figure 4. Soft tissue molding. |
At first, I utilized sutures passed intraorally through the soft tissue of the cheek and then passed through a tunnel to the temporal pocket and anchored to the temporalis fascia.
Although successful, this was somewhat arduous in terms of placing the intraoral suture at the right location in the soft tissue.
The evolving technology of barbed sutures seemed to be a logical way of engaging all layers (from periosteum to skin) in the elevated flap. Clinical indications included patients who typically were women at least 35 years old.
When the physical examination revealed a long lid/cheek junction and prominent nasolabial folds with varying degrees of soft-tissue volumetric loss, this procedure seemed appropriate.
As indicated, soft-tissue fillers (both autologous and nonautologous) could be used to augment the deficient midface. Patients with very heavy soft tissues and those with a wide interzygomatic distance may not be appropriate candidates.
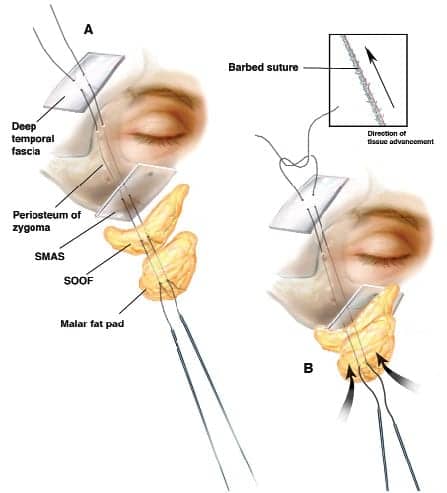
BARBED SUTURE TECHNIQUE
 |
| Figure 5. Proximal suture anchoring to soft tissue with twothread placement. |
The technique utilizes the QuillSRS bidirectional barbed sutures. Dissection begins in the temporal area and continues to the lateral orbital rim at the subfascial level.
If the individual anatomy dictates an adjustment of the lateral eyebrow, the dissection can be continued medially over the superior-lateral orbital rim, releasing the orbital ligament and the periosteum so that the lateral brow may be elevated.
The remainder of the dissection is performed intraorally, communicating the subperiosteal pocket with the temporal pocket. The QuillSRS sutures are passed from the temporal pocket, under the periosteum and engaging all layers of the cheek, exiting lateral to the nasolabial crease.
Interestingly, the distal end may be allowed to exit the skin and remain external, with an application of antibacterial ointment and nonadherent dressing for 3 days. At that time, a final adjustment can be performed to provide impressive elevation and symmetry of the midface.
Postoperative care includes placing stretchy steri-strips for 5 days of support, oral steroids, and antibiotics. The effect of this technique is to produce a “shish kabob” stacking of all of the soft tissue of the cheek.
 |
| See also “The Suture of the Future?” by N.D. Moscoe, MD, FACS, and Nicanor Isse, MD, in the April 2007 issue of PSP. |
This technique is relatively easy to master when one is familiar with subperiosteal and subfascial dissections. It can be performed with a minimal amount of equipment in a short period of time.
Morbidity is less with this technique, as the intraoral dissection is more limited than what is necessary for single- or double-suture placement.
Recovery is faster for most patients, with minimal risk due to the limited intraoral dissection. In fact, a suture is not looped into the composite flap, which may produce a temporary or a permanent motor nerve deficiency.
 |
| Figure 6. A 51-year-old female, shown here in both preoperative and 2 years postoperative, having undergone an endoscopic brow lift and subperiosteal midface lift with barbed suture suspension. |
Malcolm D. Paul, MD, FACS, is a clinical professor of surgery at the Aesthetic and Plastic Surgery Institute, University of California at Irvine. He can be reached at [email protected].
ILLUSTRATIONS AND PHOTOS COURTESY OF MALCOLM D. PAUL, MD, FACS



