In facial aging, changes are commonly represented by vectors, of which gravity, actinic damage, and natural aging contribute to soft-tissue ptosis.
Due to the effects of gravity, these vectors are predictable and common to all individuals.
A vector is defined as “a quantity that has magnitude and direction and that is commonly represented by a directed line segment whose length represents the magnitude and whose orientation in space represents the direction.”
Numerous texts and articles portray these vectors in various ways, and diagrammatically they are similar. These vectors are in reality three-dimensional but most frequently are represented in two dimensions.
The anatomy and physiology of these vectors are controversial and vary from text to text.
It is safe to say that the commonly accepted aging changes comply with basic directional vectors, and that the correction of theses vectors in the reverse direction are grossly similar for rejuvenation.
Digital technology has provided physicians with the ability to progressively age a young individual “virtually.” This is a relatively easy task and approximates true-to-life changes.
In digital aging, a youthful picture is “aged” by selectively inducing aging changes that relate to realistic vector change.1
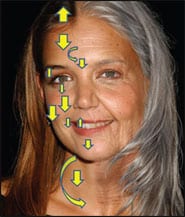
An excellent example of the art of age progression is illustrated by using a young, attractive starlet who exhibits classic signs of youth and facial volume (Figure 1).
It is interesting to see how artists render aging in any medium, digital or otherwise. They should have an understanding of the vectors that differentiate an older person from a younger one.
By examining the digital aging patient, we can appreciate the realistic vectors of aging we all deal with on a daily basis.
 |
| Figure 1. The generalized vectors of age are shown in a digitally enhanced picture of a young celebrity. |
UPPER FACIAL AGING VECTORS
In the upper face, the most noticeable vectors of aging involve the forehead, brow, and upper eyelids. Skeletal shrinkage with aging has been included as a contributor to skin laxity.
Actinic damage and generalized aging produce inferior vector aging across the brow and forehead.
The continual movement of the brow elevators and depressors produce predictable horizontal, vertical, and oblique rhytids in the brow and forehead.
Collectively, these changes in the upper face include the following:
- Graying of the hair with anterior hairline recession and elevation;
- Redundant wrinkled forehead skin;
- Ptotic brow and forehead with prominent skin around the brow depressors;
- Lateral orbital hooding and excess skin, fat, and muscle in the upper eyelids; and
- Thickening of the skin of the nasal radix.
 |
| Figure 2. Youthful areas are selected and digitally enhanced to reproduce ptotic aging vectors in the mid and lower face. |
These negative vectors are shown in the upper face of the woman in Figure 1.
To digitally recreate midface and lower facial changes, the youthful tissues are digitally altered to reflect the aging vectors, as shown in Figure 2.
The youthful areas that will become ptotic are identified as digital areas, after which the computer processes the “aging” by duplicating natural aging vectors.
 |
| Figure 3. A “before and after” image produced by simulating the vectors and changes associated with head and neck aging. |
The digital artist’s astute choice of facial areas to morph are anatomically correct—the malar fat pads, the nasal tip, and the jowls will descend with age in predictable vectors (Figure 2).
To produce these changes, the digital artist employs the same vectors and hard- and soft-tissue changes that occur in nature, which include the following:
- Lower eyelid skin dermatochalasis, with increased skin, muscle, and fat of the lower lids;
- Malar fat pad and suborbicularis oculi fat (SOOF) descent and ptosis, with accentuated nasolabial folds;
- Descent of the nasal tip;
- Jowl formation from skin changes, ligamentous laxity, and malar fat pad ptosis with resultant “marionette lines,” turned-down oral commissures, and loss of the jawline definition;
- Shortening, attrition, and yellowing of the teeth;
- Elongation of the upper lip;
- Ptosis of the chin;
- Excess and actinically damaged neck skin, with hyoid descent and platysma dehiscence; and,
- A generalized squaring of the youthful, oval face outline.
 |
| Figure 4. Surgical correction of aging vectors in the upper face by open brow lift technique. One advantage of this approach is that it allows adjustment and correction of vectors and tension across the entire brow. The left side of the photo shows the multiple skin cutbacks and key sutures. The right side of the photo shows the excess skin excised. |
When simulating aging vectors, skin changes, and other signs of aging morphs the entire face, the patient looks realistically senescent (Figure 3).
It is interesting to see how a person is digitally aged. The process can provide physicians with valuable input for the correction of the aging vectors.
SURGICAL CORRECTION OF AGING VECTORS
The discussion of aging vectors and their correction is controversial at best.
Most surgeons understand the actual complexities but explain them to their patients in generalized terms.
Many who read this article will agree with my description of vectors, whereas others will disagree. In addition, many textbooks and surgical literature are often contradictory in the area of aging mechanisms. In any event, this article is not an evidence-based analysis but, rather, a generalized means of aging vectors and their surgical correction.
Lowering the hairline with follicular grafts produces a vertical vector correction in the upper face. This is a frequent option.
The elevation of the brow and forehead provides the most dramatic reversal of upper facial aging vectors.
Although every patient is different, the generalized corrective vectors are superior and superolateral, as shown in Figure 4.
One advantage of the trichophytic brow and forehead lift2 technique is the ability to control the various vectors across the entire incision as compared to conventional endoscopic, which requires high-tension fixation in limited areas comparatively.3
In addition, the subcutaneous approach is more effective in the effacement of horizontal forehead rhytids than other techniques.
Generally, the glabellar and radix areas—as well as the maximum desired area of brow elevation—are vertical vectors, whereas the lateral brow is a more superolateral vector.
Most patients do not desire significant medial brow elevation, as it adds to an unnatural appearance.
Regardless of the operative technique or approach, all brow and forehead lifting procedures have the same intention, which is to reverse the negative or inferior vectors of upper facial aging.
REVERSING MIDFACIAL AGING VECTORS
Although aging vectors are most often represented in two dimensions, in reality they all have three-dimensional components, which in facial rejuvenation are represented in volume loss and its restoration.
Cosmetic surgeons should have a keen appreciation of volume restoration, which is reflected in their surgical procedures.
For example, midface rejuvenation can include skin resurfacing, injectable facial fillers, midface lifting procedures, cheek implants, or a combination thereof.
 |
| Figure 5. This patient is shown before and after midfacial rejuvenation with cheek implants, minifacelift, and upper blephroplasty. The center image illustrates the generalized desired vectors in the correction of midface aging. The yellow arrows indicate superior and superolateral vector reversal. The red arrow represents the third dimension of inflation, or volume increase. |
The desired result is to improve the patient’s gaunt appearance, which could be caused by malar fat pad and SOOF descent; to restore curves of youthful volume; and, hopefully, to improve nasolabial fold esthetics.
Bringing volume back to the deflated midface is similar to the effect of breast implants. Inflation and superior and superorlateral repositioning of ptotic midface soft tissues are small procedures that can make absolutely huge changes in the patient’s overall aesthetic appearance (Figure 5).
The patient shown in Figure 5 underwent a mini-facelift, upper blepharoplasty, and the placement of submalar silicone cheek implants.
Although each separate procedure produced made improvements to the patient’s aging face, the restoration of midfacial volume is truly what makes this patient look younger. (Failure to address the midfacial vectors would have been a serious disservice to this patient.)
CORRECTING AGING VECTORS IN LOWER FACIAL REJUVENATION
 |
| Figure 6. The direction of pull on facelift skin flaps is perpendicular to the incisions. The vertical temporal incision (left image) does not provide the degree of control of skin vectors as does the more geometric incision (right image), which preserves the temporal tuft and also provides more flexibility to adjust vector position. |
Although close attention is required to how you reposition soft tissues in any aesthetic procedure, facelift surgery requires profound control of aging-vector repositioning in order to provide a natural-looking result.
Few aesthetic procedures are as sensitive to directional pull as this one. Small miscorrections can make very apparent differences that scream of an unnatural facelift.
Vector control in facelift surgery begins with the incision planning, as the vector direction of pull should be perpendicular to the incision.
Though many surgeons prefer a simple vertical incision in the temporal area, this incision can be problematic in several ways.
With the vertical temporal incision, the surgeon has much less control of the temporal tuft position, and attempting to pull excess skin in a superolateral vector can induce significant temporal balding—another stigma of a bad facelift.
By using a more geometrically designed incision, one can preserve the temporal tuft as well as enable vector control in more directions, when compared to the purely vertical incision (Figure 6).
Directional control is also important in the deeper layers of the rhytidectomy. Whether or not you use placation or imbrication techniques, close attention to vector management is imperative.
 |
| Figure 7. The SMASectomy shown in the left image has an arrowhead shape. When reapproximating the SMAS borders, the surgeon has increased control of the SMAS pull when compared to a rectangular SMAS excision. |
I believe that SMASectomy procedures provide the best means of controlling vectors in the deeper plane.
By excising a strip of SMAS from the malar region and into the lower cervical regions, the surgeon can pull the SMAS as a unit using multiple vectors in multiple directions across the entire length of the SMASectomy site.
The combination of vectors of pull can provide enhancement of the midface, the cheek and jowl region, and the upper cervical area with a single SMASectomy excision.
SMASectomy4 excises a simple rectangle of SMAS and allows pull in multiple directions.
By adding various geometrics to the SMASectomy incision, an increased and diverse vector control can be achieved as shown in Figure 7.5
Employing a more geometric SMASectomy incision may not always be necessary, especially in younger patients. However, in many patients the added vector control is advantageous.6
 |
| Figure 8. Facelift patients with significant skin wrinkling are very prone to a noticeable “wind tunnel look,” revealing that proper skin vectors were not followed by the surgeon. Laser resurfacing can mitigate this problem. |
VECTOR CONTROL IN SKIN REPOSITIONING
The final step in facelift surgery is skin repositioning and excision, which is probably the most critical step in producing a naturally appearing facelift result.7
Although this is a very basic tenet of rhytidectomy, some physicians are obviously unsure or unclear about this step. For example, I have seen patients who had their skin pulled and sutured in an unnatural vector.
This “wind tunnel look” stands out as one of the most notable negative stigmata of rhytidectomy (Figure 8). This is a problem in patients with significant skin wrinkling, as changing wrinkle direction can call attention to the unnatural vector of pull.
Although laser resurfacing can ameliorate this problem, all patients require (and deserve) well-planned directional skin pull and suspension.
When making skin cutbacks and placing key sutures, you should closely observe the vector of pull in order to produce the most natural-looking result.
 |
| Figure 9. Manipulating the skin vector of pull can be critical to the final appearance in facelift surgery. The flap can be suspended in multiple directions, and the surgeon and staff must recognize which vector is most effective and natural. The left image shows a pure horizontal vector, and the right image shows a combined vector with superolateral pull. Somewhere between theses vectors lies the optimum direction of tension for the patient. |
Whereas the average direction of skin pull is superior and lateral, each patient is different, and the skin should be suspended in multiple vectors so that you can see which position provides the most effective and natural tension (Figure 9).
Frequently, I suspend the flaps several times. As the vector of pull can change while making various skin cutbacks, it can be advantageous to cut the key sutures and resuspend the flap in a different vector to ensure the most effective and natural pull.
Some rhytidectomy techniques employ a more vertical vector, and these authors obtain successful results.8
One potential problem associated with more purely vertical skin-pull vectors is the bunching that can occur in the posterior auricular region, especially if a short-scar technique is employed.
As with all other procedures, numerous techniques and individual surgical preferences can produce aesthetic outcomes, and there is no universal consensus of technique.
 |
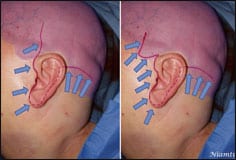
| Figure 10. A before-and-after image showing the generalized direction of vector pull utilized in the correction. |
CONCLUSION
The concept of vectors of aging and their surgical correction is a controversial means of describing aging and surgery.
Part of the difficulty lies in using a two-dimensional system to describe a three-dimensional process.
Evidence-based studies are emerging, with technologies such as CT scan, 3D photography, and digital imaging to better quantify aging changes.9
This article summarizes how directional vectors apply to gravity, aging, and aesthetic facial surgery. Appreciation for the mechanics of aging and its related correction is essential to provide natural-appearing surgical results.
 |
| Figure 11. A before-and-after image of a patient with significant facial ptosis. Close attention to directional pull is essential for natural-looking results. |
Figure 10 shows a before picture with the anticipated correctional vectors (blue arrows indicate inflational volume) and the patient’s actual postoperative result.
Figure 11 shows a patient who underwent a facelift with bilateral SMASectomy, submalar cheek implants, upper and lower blepharoplasty, and full-face CO2-based laser resurfacing.
The patient would have benefited from a brow and forehead lift, but declined the option.
Other than her brows, reversing the directional ptosis and adding volume to the midface have successfully corrected the main vectors of aging.
Joseph P. Niamtu III, DMD, is a board-certified oral and maxillofacial surgeon in private practice in Richmond, Va. He can be reached at .
REFERENCES
|
See also “Embrace the Midface” by Allison T. Pontius, MD, Edwin F. Williams III, MD, FACS, and Alain Polynice, MD in the April 2006 issue of PSP. |
- www.exguides.org. Accessed March 20, 2008.
- Mayer TG, Fleming RW. Fleming-Mayer flap (modified after Juri) forehead lifting. In: Aesthetic and Reconstructive Surgery of the Scalp. St Louis: Mosby; 1992.
- Niamtu J. Endoscopic brow and forehead fixation: all that and more. Plast Reconstr Surg. 2005;115(1):357-358.
- Baker DC. Minimal incision rhytidectomy (short scar facelift) with lateral SMASectomy: evolution and application. J Aesthetic Surg. 2001;14-26.
- Abramo AC, Oliveira VR. The “lazy S-shaped” plication of the SMAS-platysma musculoaponeurotic system: a 10-year review. Aesthetic Plast Surg. 2000;24(6):433-439.
- Cárdenas-Camarena L, González LE. Multiple, combined plications of the SMAS-platysma complex: breaking down the face-aging vectors. Plast Reconstr Surg. 1999;104(4):1093-1100; discussion 1101-1102.
- Hamra ST. Prevention and correction of the “face-lifted” appearance. Facial Plast Surg. 2000;16(3):215-229.
- Tonnard PL, Verpaele A, Gaia S. Optimising results from minimal access cranial suspension lifting (MACS-lift). Aesthetic Plast Surg. 2005;29(4):213-220.
- Barrera JE, Most SP. Volumetric imaging of the malar fat pad and implications for facial plastic surgery. Arch Facial Plast Surg. 2008;10(2):140-142.


