PHOTOS COURTESY OF JOSEPH NIAMTU III, DMD

In cosmetic surgery, you can certainly find more “sexy” operations than the repair of the lowly earlobe. Nonetheless, this is a commonly requested operation. As with all procedures, large and small, to perform it correctly requires finesse and understanding of what it takes to obtain consistent and aesthetic outcomes. Anyone can excise a fistula and sew the lobe back, but those who do it best have an understanding of what small alterations compensate for common mistakes.1,2,3
Earlobe tears are extremely common and mostly seen in female patients. With the increase in male piercings, as well as extreme dilations and piercings, it has become even more common and challenging to perform this operation on both sexes.
Common causes of lobe tears include continued wearing of heavy, pendulous earrings; trauma from snagging earrings on clothes; hairbrushes; telephone cords; assault; domestic abuse; and babies pulling on shiny objects dangling from earlobes. Some patients present with freshly torn lobes, but the vast majority of earlobe tears are chronic and the patient has had the condition for years.






Figure 1. This image shows partial (left), full (center) and multiple (right) earlobe tears.
Figure 2. Simple fistula excision and repair of a partial tear that includes the inferior one-third of the lobe can produce a pointed lobe and should be treated by violating the interior lobe border to obtain better approximation and form.
Earlobe tears can be classified into partial, full, and multiple tears. Partial tears are usually a simple elongation of the original piercing and bother patients as their earrings no longer sit correctly or the added weight produces an elongated opening. Full tears represent a violation of the inferior lobe border and can be multiple in nature (Figure 1).




Figure 3. A partial tear that extends to the lower one-third of the lobe should be converted to a total tear to optimize the cosmetic result and prevent “pointing” of the lobe.
Figure 4. Placing offset sutures to control the position of closure can prevent pointing of lobe when closing an incomplete defect.
Many authors have offered techniques for improved aesthetics with earlobe repair. Earlobe repair is a simple 10- to 15-minute procedure performed with local anesthesia. The earlobe is injected with local anesthesia and, for partial tears, the elliptical tear is excised and resutured with a 6-0 fast-absorbing gut suture. This works well if the tear does not include the inferior 1/3 of the lobule. If the sagging hole (ellipse) extends into the lower 1/3 of the lobe, a simple excisional repair will frequently produce a pointed lobe (Figures 2, 4, and 5). For this reason, lobe tears that extend into the lower 1/3 of the lobe are converted to a full tear by incising the inferior border of the lobe and creating a “V” excisional defect, which is easily closed and can control the inferior lobe border form and continuity.




Figure 5. A pointed or stepped lobe can be easily recontoured with a radiowave ball electrode or CO2-based laser.
Figure 6. The ellman fine wire “Varitip” electrode or CO2 laser incisional handpiece provide numerous advantages over other incisional methods for earlobe repair.
If a pointed lobe is apparent during the repair, the surgeon can control the point by positioning the sutures with an offset to close the defect without pointing the lobe (Figure 4). In addition, Vujevich and Obagi4 have described a purse string suture to prevent pointing.



Figure 7. This image shows a preincision photo (A), the parallel inferior lobe incision (B), and the exisional defect(C).


Figure 9. Wedge resection is a simple technique for the reduction of large earlobes. A wedge of excess lobe is excised with primary closure. Although an acceptable scar usually results, CO2 laser resurfacing can be performed to improve the surgical scar.
Figure 8. Everting the inferior lobe with a mattress suture will decrease the notching defect seen with healing contraction.
Finally, in the case of a pointed lobe (intraoperatively or after healing), the pointed inferior lobe can be reshaped using a radiowave ball electrode or CO2-based laser to flatten the pointed anatomy (Figure 5).
COMPLETE TEARS
Excising the border of the “V” defect and resuturing treats complete tears, which are the most common. Although quite simple, numerous pearls will prevent common pitfalls of lobe repair.
Border scar incision can be completed with scalpel and scissors, but is greatly simplified by using a radiowave microneedle (Ellman International, Ocean Side, NY) or a CO2-based laser (Lumenis Inc, Santa Clara, Calif). The advantages of these modalities include simultaneous cutting and coagulation, a “pressure-less” incision (which is advantageous with a mobile structure), and their ability of very precise control due to the fine gauge of the cutting wire (Figure 6). The laser also works quite well in this application.
The first important action is to excise the inferior lobe surface so that the approximating surfaces will be completely parallel to one another. This is accomplished by making sure enough of the inferior lateral surface is included in the incision (Figure 7).
A critical step is to precisely line up the inferior lobe border with a 6-0 suture in a similar manner as vermilion/cutaneous approximation in lip surgery. Failure to properly align the lobe can result in notching or an unaesthetic result.
Hemostasis is a concern with lobe repair. The earlobe is extremely vascular, and the local anesthetic can constrict vessels that can bleed later. Using a micro bipolar forceps is efficient for hemostasis. Although some surgeons utilize subcutaneous sutures, I have not found them necessary.
The single most important step in earlobe repair is crafting a smooth and natural inferior lobe border. The most common complication of earlobe repair is retraction—or notching—of the repaired lobe. This involves inexact approximation of the lobe border and/or wound contraction. Regardless of the cause, this common pitfall can be avoided by everting the inferior lobe border to account for wound contraction (Figure 8).
Having to go without earrings for the healing period is unfavorable for some patients, and immediate repair and piercing can be easily performed.
This technique is performed by completing the repair and then placing a dedicated piercing stud through the suture line. Standard earrings are not a good choice, as their posts are shorter and can cause pressure necrosis on the repair.





Figure 10. Megalobe can also be treated by marginal resection of the hypertrophic lobule. Picture A shows the excess lobe being marked while B shows the excess tissue excision with a “V” pattern to produce a thinner border and hide the scar. C shows the sutured lobule with the suture line placed at the inferior lobe to produce a hidden scar.
Figure 11. A complete earlobe tear is shown before and after repair.
One disadvantage of immediate repair and piercing is that it is difficult to accurately place the earring due to local anesthesia engorgement, edema, and the position of the suture line. If immediate piercing is not performed, the lobe should be allowed to heal 30 days prior to repiercing.
EARLOBE REDUCTION
Megalobe is a condition that can be hereditary or, in some cases, a result of aging. Large, pendulous earlobes are unattractive to many patients, and requests for lobe reduction are common in cosmetic surgery practices.
Numerous techniques exist for earlobe reduction. The most common consist of a “wedge” or other geometric reduction, as well as simple peripheral lobule trimming. Again, this procedure is usually performed with local anesthesia and heals with minimal scarring.
To perform the wedge-type reduction, a triangle of hypertrophic lobe is marked and injected with local anesthesia. The excess is removed, and the same principles of the aforementioned lobe approximation techniques are applied. An impressive amount of lobe excess can be excised and is sometimes underestimated by novice surgeons. Figure 9 shows a typical wedge resection technique.
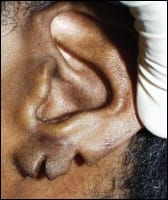



Figure 12. A multiple earlobe tear is shown before and after repair.
Figure 13. A hypertrophic earlobe is shown before and after marginal border excision.
Peripheral margin reduction techniques are simply performed by outlining the desired limits of the new lobe and trimming the excess. Although scissors or scalpel can be used, I prefer the radiowave microneedle for this procedure, as the tissue contact is light and almost comparable to laser incision. The incision should be designed to hide the final scar at the inferior border or on the medial surface of the lobe. By incising in a manner that allows a longer lateral flap and shorter medial flap, the suture line is hidden on the medial surface. Figure 10 shows the sequence of peripheral margin reduction.

On The Web!
See also "Solving the Scar Problem" by Jerome D. Chao, MD, in the March 2006 issue of PSP.
COMPLICATIONS
Significant complications are rare with this simple procedure and usually involve pointed lobe, stepped lobe, and unfavorable scarring. Severely stepped or pointed lobes may require a revision procedure to correct. As mentioned earlier, a radiowave ball electrode is useful to recontour pointed or stepped lobes. For unfavorable scars, CO2 laser resurfacing is an excellent option for revision to smooth and blend the scar.
Joseph Niamtu III, DMD, is a board-certified oral and maxillofacial surgeon. His practice in Norfolk, Va, is limited to cosmetic facial surgery. He can be reached at .
REFERENCES
- Niamtu J. Eleven pearls for cosmetic earlobe repair. Dermatol Surg. 2002 Feb;28(2):180-185.
- Niamtu J. Repair of cleft earlobes. In: Cosmetic Facial Surgery Oral and Maxillofacial Surgery Clinics of North America. Philadelphia: WB Saunders; 2000;12(4):781-789.
- Niamtu J. Surgical repair of cleft earlobe. J Oral Maxillofac Surg. 1997;55(8):886-890.
- Vujevich J, Obagi S. Repair of partial earlobe cleft using a “purse-string” repair. Dermatol Surg. 2006;32(4):969-971.