 |
Blepharoplasty patients who have experienced a pleasing aesthetic outcome but complain of ocular symptoms can be a challenge for most surgeons, particularly when the cause of their complaint is not obvious.
Following an elective, aesthetic surgery, a vision complaint—particularly one that disrupts daily function—will most certainly lead the patient to voice displeasure and want a solution.
At times, the smallest lid problem can cause a larger magnitude of ocular discomfort, visual changes, and/or (on rare occasions) a vision-threatening problem. As with any postsurgical complication, recognition and timely management keep both the patient and surgeon satisfied.
Frequently, I consult with blepharoplasty patients who underwent surgery elsewhere and developed ocular symptoms in the immediate postsurgical period or even months after their surgery. At times, my own patients have similar problems with which to contend.
Problems, such as an ectropion following lower blepharoplasty, are not the diagnostic challenge here. Instead, the challenge is in discerning more subtle changes in lid function and position affecting the ocular surface.
 |
| Figure 1. Punctoplasty opens the closed or narrowed puncti (plug hole) of the lower eyelid, allowing the patient’s tears to drain into the outlet pipe and into the nose and down the throat. |
As an oculoplastic specialist with a background in ophthalmology, I am familiar with slit lamp biomicroscopy, an examination tool generally not used in nonophthalmic practices. The slit lamp allows for a magnified evaluation of the ocular surface and adnexal structures, such as the lacrimal puncta, which are not visible to the naked eye.
DRY AND WET
By far, the two most common functional eye complaints encountered after blepharoplasty are the “wet eye” and the “dry eye.”
In dermatology, the adage of, “If it’s wet, dry it, and if it’s dry, wet it,” may be common, but in aesthetic surgery, that saying does not always apply when it comes to ocular surface issues.
A wet eye (epiphora) can diminish central vision, similar to a wet windshield affecting a driver’s visibility. The lid skin often becomes macerated from constant Kleenex wiping. However, if there is complete lid closure and a complete blink, epiphora is usually not a visually threatening issue.
By far, poor lid-to-globe apposition and lower-lid laxity—with or without punctal stenosis—account for excess tears in most patients. Patients who develop even transient lower-lid margin ectropion after lower blepharoplasty can have the lower lacrimal puncta narrow in caliber or closed completely. The lower lid can look well positioned, but with the puncta closed, tear egress will be diminished.
 |
 |
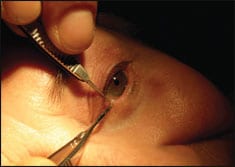
| Figiure 2. An example of lagophthalmos with poor Bell’s phenomena. | Figure 3. Dilation of punctum is useful treatment when mechanical, inflammatory, or infectious processes obstruct normal tear drainage. |
The identification of punctal stenosis can be made with surgical loupes. Simple dilation using a punctal dilator following a topical anesthetic application may be the solution. On the other hand, postoperative lower-eyelid wound contracture, leading to a “stiff” or relatively immobile and/or retracted lower lid—if mild—will typically respond to simple vertical lid massage.
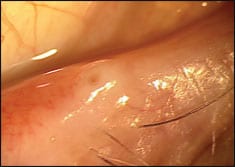 |
| Figure 4. An example of punctual stenosis. Several mechanisms may cause punctual stenosis, including inflammation from infection, topical drug toxicity, and viral infection. |
In the case of more severe lower-lid retraction, placement of a Frost suture for 5 to 7 days, though inconvenient for the patient, can give the lower lid an additional 1 mm to 2 mm of elevation—if performed in a timely manner.
If focal cicatricial bands are present, a 16- or 18-gauge needle can be used for lysis while the lid is on stretch with the Frost suture. The same needle can then be used to infiltrate triamcinolone into the affected tissue. This can be performed in office with local anesthetic in most cases.
An incomplete or weakened blink from postsurgical wound contracture and/or orbicularis muscle dysfunction may cause tearing and simultaneous corneal drying.
In areas of the country where dry, low humidity is experienced in the winter months, this risk is amplified. Any physician who manages patients with paralyzed faces knows all too well that corneal drying is a far greater concern in winter than in summer. I have come to recognize, via the venerable school of hard knocks, that dry eye or ocular surface disease patients who are entertaining blepharoplasty should plan their surgery for summer months, when the air is humid. They will experience far fewer complications than when they undergo the surgery in the middle of winter.
What can the nonophthalmic blepharoplasty surgeon rely on as warning flags of a potentially serious dry eye?
THE RIGHT APPROACH
|
See also “The Open Brow Lift Revisited” by Joseph Niamtu III, DMD, in the January 2006 issue of PSP. |
 |
When teaching blepharoplasty, I always emphasize that you should evaluate Bell’s phenomena and document it in your preoperative evaluation. As this can be quite variable, any patient with minimal upward eye movement with lid closure should be flagged as one who will not be able to tolerate lagophthalmos, no matter how mild.
In addition, a simple office examination to perform is the light reflex. A dull corneal reflex is indicative of a dry eye and cornea versus the crisp, sharp reflex indicative of a well-hydrated cornea.
A cornea “spot” visible during your external examination should be managed by an ophthalmologist promptly.
By far, the best advice for a non-ophthalmic blepharoplasty surgeon is to be vigilant in your initial exam. Also, obtain a detailed history of contact lens intolerance, dry eye, blepharitis, and artificial tear use (which should prompt an eye examination if you have any suspicion of a compromised ocular surface); and establish a relationship with a local ophthalmologist who can help you if your patients return to you with eye complaints.
Jeffrey J. Zuravleff, MD, is an oculoplastic-orbitofacial surgeon in private practice in Richmond, Va. He can be reached at .



