|
Patients seeking aesthetic surgery are looking for the quick fix. Most expect to walk into the operating room, have their surgery done today, and return to work tomorrow.
Currently, a large majority of your prospective clients are seeking a procedure that will remove fat; slim the waistline; and lift, tuck, or tighten the skin.
One of the most common reasons that patients seek plastic and aesthetic surgery is body contouring—more specifically, lipocontouring.
Liposuction is no longer the flattening out of a bulge of unwanted fat. It is the reduction of an unsatisfactory shape to a new, smoother contour line.
This extremely popular procedure is not without risks. Potential risks and complications include infection, seroma, hematoma, contour irregularities, asymmetry, deep venous thrombosis, pulmonary embolus, fat embolus, and death.
For these reasons, it is essential to follow general guidelines set forth by the American Society for Aesthetic Plastic Surgery and/or the American Academy of Cosmetic Surgery.
If these guidelines are followed, this can be a safe and successful surgery with minimal downtime and few associated risks.
A TWO-WAY STREET
No matter what technique or instrumentation is used, body contouring with liposuction is no easy task and requires patience, skill, and an artistic eye.
The patient seeking liposuction is a unique challenge to the surgeon—many of them expect a lot from the surgeon with little effort of their own.
As a result, it is imperative that you, prior to surgery, discuss potential risks and complications with the patient. He or she needs to know that the likelihood of contour irregularities will increase with poor skin tone and quality, as well as with the presence of cellulite.
Inform patients that lipocontouring does not treat cellulite and that it is not a form of weight loss.
Many times, I offer the analogy of fat being like feathers—one has to bag a lot of feathers to get the bag to weigh 1 pound. Fat is similar.
 |
 |
 |
 |
 |
 |
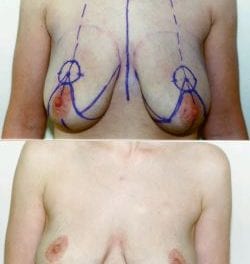
| Figure 1. Preoperative and 6 months postoperative photos of a 34-year-old Caucasian female who received lipocontouring of the trunk and bilateral upper arms, combined with bilateral breast augmentation and adherence to recommended postop lifestyle changes. | |
Liposuction is not a form of weight loss but, rather, a slimming and contouring procedure that will eventually allow the patient’s clothes to fit more comfortably—lipocontouring.
Also, I ask patients to be realistic in their goals—he or she must understand that it is impossible to achieve perfect symmetry. In all patients, I point out their asymmetries during initial consultation.
I ask them to make a commitment. The patient is informed that I am making a commitment to them and that they must make a commitment not only to me but to themselves as well.
The patient must understand that liposuction is going to succeed as long as he or she makes lifestyle changes following the procedure, including improved eating habits and daily exercise programs.
If the patient can apply these lifestyle changes and lose 2 to 5 pounds following the procedure, then the rewards are only greater.
I challenge patients to change their dietary habits by increasing whole grains, including wheat bread, brown rice, and sweet potatoes. They should cut out anything that is “white” in their current diet, such as white bread, white rice, and white potatoes.
In addition, I ask patients to increase their daily food intake to six small meals per day, which limits their daily intake of fat to less than 30 grams per day.
Combined with daily exercise, this change will increase the patient’s metabolism and allow for improved aesthetic results following lipocontouring.
After the patient has accepted my challenge for lifestyle changes, they are then ready for surgery. An example of this can be seen in Figure 1.
| Table 1. Modified Klein’s Tumescent Solution | |
| 1,000 cc | Normal Saline |
| 50 cc | Lidocaine 1% Plain |
| 2 cc | Epinephrine 1:1000 |
Following lipocontouring and breast augmentation, this 34-year-old patient made a lifestyle change and achieved obvious results in less than 6 months.
SURGICAL TECHNIQUE
Options for surgery include local anesthetic alone, local anesthetic with combined intravenous sedation, or general anesthetic.
The physician and anesthesiologist make this decision and many times take into account the patient’s anxiety level and general level of pain tolerance.
After the anesthesia has been determined, the patient is marked in a standing position in the preoperative holding area.
After general markings are complete, the patient is taken to the operatory and administered anesthesia.
Upon consent of the anesthesiologist, the patient is placed into the appropriate anatomic position to adequately treat the area of lipodystrophy. Betadine solution is used to prepare the patient.
After sterile draping, tumescent solution is infiltrated into the selected area through an 11-blade stab incision.
The mixture used is based on the Klein technique, as seen in Table 1. After adequate epinephrine effect—at about 12 to 18 minutes—lipocontouring can then be carried out using a variety of liposuction equipment.
My personal preference is the use of ultrasonic-assisted liposuction (UAL) combined with the mechanical effect of the Power Assisted Lipoplasty (PAL) system by MicroAire Surgical Instruments LLC, Charlottesville, Va, which is a reciprocating cannula for lipoplasty.
I tend to use UAL to “pretunnel” and emulsify fibrous areas that are usually seen posterior to the midaxillary line, such as the superior hip folds extending to the posterolateral flanks, breast folds, etc.
In addition, UAL aids in providing mild skin tightening and is, therefore, useful to treat areas with mild to moderate skin laxity—as can be seen in the submental area and the bilateral upper arm region.
For all other areas, I prefer to pretunnel using a 4-mm or 5-mm cannula that is not connected to a vacuum.
This allows for rapid breakup of fat cells and fibrous areas.
Without suction, pretunnelling creates much less fatigue on the surgeon.
Following pretunnelling techniques, I use PAL to remove the majority of volume from the selected treatment areas.
During all treatments, it is extremely important to be cognizant of the volume of fat being removed. Too little fat results in minimal results, and too much results in an extremely unhappy patient due to the potential risks of contour irregularities and skin burns associated with UAL.
The easiest way to maintain a happy medium is via the “pinch” test. Pinching the skin and subcutaneous tissues allows the surgeon to determine the amount of fat removed during the procedure.
The recommended final pinch test results should be greater than 1 cm following lipocontouring.
Therefore, it is recommended that the pinch test be performed preoperatively to truly assess the remaining amount of fat.
During the procedure, frequent pinching of the tissue will allow the surgeon to gauge the amount of fat removed compared to the preoperative pinch volume.
Remember, never remove fat that results in a pinch test equal to less than 1 cm.
Following completion of the surgical procedure, all incisions are closed in a multilayer fashion using 4.0 monofilament absorbable suture subcuticularly and 5.0 polypropelene in a simple, interrupted fashion at the skin edge.
Sterile dressings, combined with external compression garments, are then applied. The patient is sent home on prophylactic broad-spectrum antibiotics combined with light pain medications for 5 days.
THE FINAL RESULTS
When the patient is discharged, he or she is given a list of do’s and don’ts to follow for the next 3 to 4 weeks.
|
See also “A Fine Balance” by Joseph P. Niamtu III, DMD in the July 2007 issue of PSP. |
These instructions include the continued use of the compression garment 23 hours per day for the first 2 to 3 weeks; thereafter, the patient should wear it only during vigorous activity for another 3 to 4 weeks.
The patient meets with our massage therapist at about 10 days postoperatively for a 1-hour lymphatic massage. At that time, the patient is instructed on home massage of all surgically treated sites, and is also encouraged to continue with routine lymphatic drainage massages (performed by our massage therapist).
Finally, the patient is again encouraged to be realistic in his or her expectations, and to understand that the final result may not be seen before 6 months due to persistent swelling.
Michael S. Kluska, DO, FAACS, FACOS, is a dual board-certified plastic and reconstructive surgeon and general surgeon in private practice in Greensburg, Pa. He is a graduate of Washington & Jefferson College with an undergraduate degree in art. He attended medical school at Des Moines University. Kluska can be reached at .